The Launch of Shenzhou-23: A One-Year Orbital Mandate
On Sunday night, May 24, 2026, at precisely 11:08 PM Beijing Time (15:08 GMT), a three-stage Long March 2-F carrier rocket ignited on its pad at the Jiuquan Satellite Launch Center in the windswept Gobi Desert. Atop the booster sat the Shenzhou-23 crewed spacecraft, carrying three Chinese astronauts into a night sky illuminated by a column of propellant exhaust. Just 3.5 hours later, after an automated rapid rendezvous and docking sequence, the spacecraft successfully linked with the core module of the Tiangong space station, orbiting approximately 400 kilometers (248 miles) above the Earth.
The mission crew is a striking blend of scientific expertise and historic firsts. It is commanded by Zhu Yangzhu, a 39-year-old space engineer; piloted by Zhang Zhiyuan, also 39, a former military aviator; and rounded out by 43-year-old payload specialist Lai Ka-ying (known in Mandarin transliteration as Li Jiaying), a computer forensics expert and former Hong Kong police officer who is the first astronaut from Hong Kong to enter space.
Yet, the headline of the Shenzhou-23 mission lies not in its launch mechanics or its diverse crew roster, but in its scheduled duration. For the first time in the history of China’s space program, one of these three newly arrived astronauts is slated to remain aboard the Tiangong space station for a continuous, uninterrupted year—365 days in orbit.
This historic one-year orbital stay marks a major shift in Beijing’s space flight operations. Since the construction of Tiangong began in earnest in 2021, China Manned Space Agency (CMSA) crews have adhered strictly to standard six-month (180-day) rotations. Pushing an astronaut to a full 12 months in microgravity is a deliberate and mathematically rigorous stress test of human physiology.
The primary biological bottleneck of long-duration spaceflight is the deterioration of the human skeleton. Beijing is currently racing against the United States to land humans on the Moon before 2030 and establish a permanent base, the International Lunar Research Station (ILRS), by 2035. Because of these deep-space ambitions, understanding and mitigating astronaut space bone loss has transformed from a niche scientific inquiry into an absolute structural prerequisite for long-duration operations.
Standard Chinese Space Rotation: 180 Days (6 Months)
Shenzhou-23 Deep-Space Stress Test: 365 Days (12 Months)
Target Crewed Moon Landing: By 2030 (1,300+ Days Away)
Target Permanent Lunar Base (ILRS): By 2035The Nonlinear Physics of Prolonged Weightlessness
"Assigning an astronaut to a one-year in-orbit stay is not simply doubling the duration of two six-month missions," noted CMSA spokesperson Zhang Jingbo during a pre-launch press conference at Jiuquan. From a systems engineering and human-factors perspective, the physiological toll of microgravity on the human body is a highly complex, non-linear phenomenon.
On Earth, human biology is continuously calibrated to a constant gravitational acceleration vector of $1g$ ($9.81 \text{ m/s}^2$). Under this force, the skeletal system experiences daily mechanical loads that trigger piezo-electric signals and fluid shear stress within the bone matrix. These forces act as a biological command signal, instructing specialized cells to maintain bone density and structural strength.
In low-Earth orbit (LEO), astronauts exist in a continuous state of freefall, effectively rendering gravity null ($0g$). Without the mechanical loading of body weight and locomotion, the human body registers the skeleton as an unnecessary, energetically expensive luxury. The body rapidly begins to demineralize its own support structures.
Earth (1g Environment):
Mechanical Load ──> Osteocyte Signaling ──> Bone Deposition = Bone Resorption (Homeostasis)
Orbit (0g Environment):
No Mechanical Load ──> Suppressed Signaling ──> Bone Resorption >> Bone Deposition (Severe Decay)The medical challenge of a one-year mission is that physiological decay does not follow a linear path toward a clean plateau. During the first 30 to 60 days of spaceflight, the body undergoes an acute phase of adaptation. Fluids shift cranially, blood volume decreases by up to 15% to 20% to compensate for increased upper-body pressure, and muscles that support posture—such as those in the calves, thighs, and lower back—begin to atrophy, losing up to 20% of their mass within just two weeks.
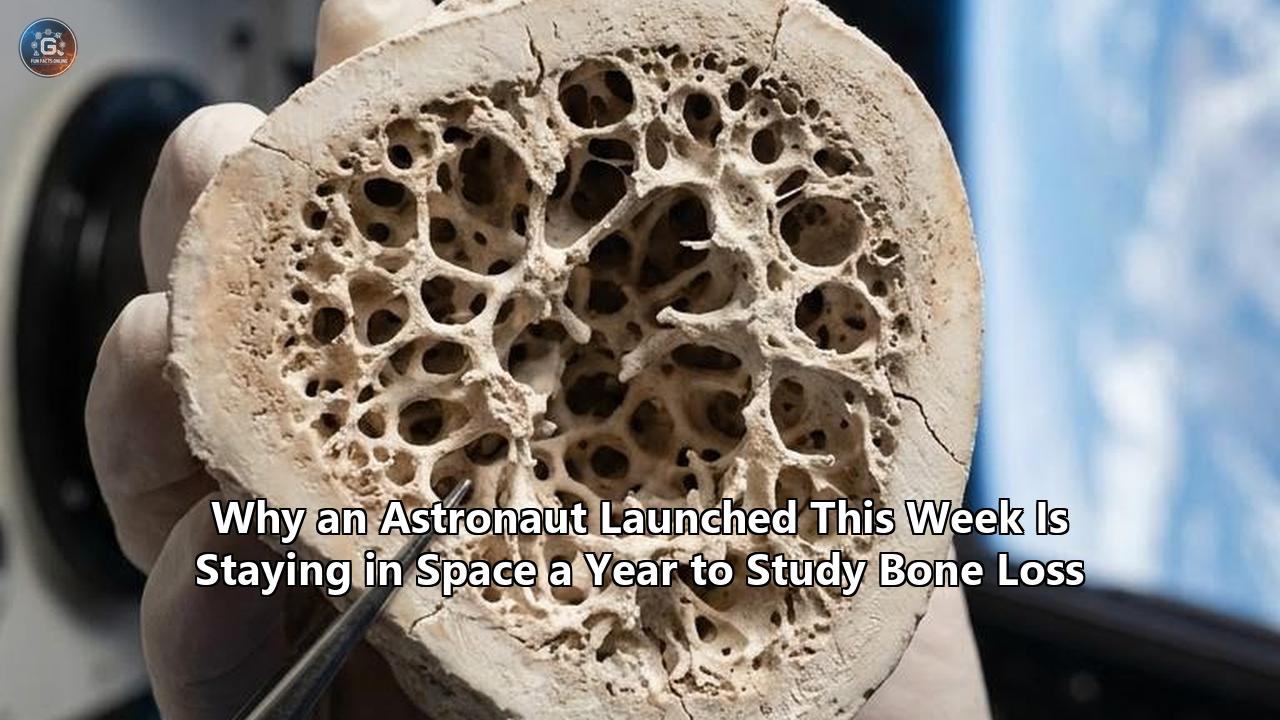
As a mission extends past the 180-day mark, bone demineralization continues unabated. Unlike muscle tissue, which can be partially stabilized through high-intensity resistance training, the loss of trabecular (spongy) bone microarchitecture continues to accumulate.
When an astronaut crosses the 300-day threshold, the systemic changes to their skeleton become increasingly severe. The continuous dumping of calcium into the bloodstream spikes the risk of painful kidney stones (nephrolithiasis), while the structural degradation of weight-bearing joints increases the risk of fractures.
By subjecting a Shenzhou-23 crew member to a 365-day orbital stay, Chinese scientists are seeking to map the precise mathematical curve of this long-term skeletal decay. Collecting this data is essential for designing life-support, pharmaceutical, and exercise protocols that can preserve human health on missions that will far exceed the bounds of Earth's protective magnetosphere.
The Quantitative Mechanics of Skeletal Demineralization
The baseline metrics of astronaut space bone loss are well-documented. Decades of research compiled by NASA, Roscosmos, and European agencies reveal that in a microgravity environment, astronauts lose an average of 1.0% to 2.0% of their bone mineral density (BMD) for every 30 days spent in space.
To put this number into perspective, it is helpful to compare it to the rate of bone loss associated with severe bone-wasting diseases on Earth. A postmenopausal woman on Earth who has been diagnosed with clinical osteoporosis, and is considered at high risk for spontaneous fractures, loses bone density at an average rate of 1.0% to 2.0% per year.
An astronaut aboard a space station experiences this exact same level of skeletal demineralization in just one month. Spaceflight effectively accelerates skeletal aging by a factor of 12.
| Subject Population | Average Rate of Bone Mineral Density (BMD) Loss | Timeframe |
|---|---|---|
| Terrestrial Healthy Adult | $0.0\%$ (Stable Homeostasis) | Per Year |
| Terrestrial Osteoporosis Patient | $1.0\%$ to $2.0\%$ | Per Year |
| Astronaut in Microgravity ($0g$) | $1.0\%$ to $2.0\%$ | Per Month |
This skeletal decay is not distributed evenly across the human body. The bones of the skull, jaw, and upper extremities (such as the arms and wrists) experience minimal loss because they do not serve a primary load-bearing role against gravity on Earth.
Instead, the demineralization is heavily concentrated in the lower half of the skeleton—the weight-bearing bones that bear the brunt of terrestrial locomotion. The most severe bone loss occurs in:
- The calcaneus (heel bone)
- The distal tibia and fibula (shinbones)
- The femoral neck and trochanter (hip joints)
- The pelvis
- The lower lumbar vertebrae
On a standard six-month (180-day) orbital mission, an astronaut’s lower vertebrae and hip joints will lose approximately 6% to 12% of their total bone mass. On a one-year (365-day) mission like the one initiated by the Shenzhou-23 crew, that cumulative loss can easily climb to 12% to 24% if left unchecked by aggressive interventions.
6-Month Mission: [████] 6% to 12% Bone Mass Lost (Serious)
12-Month Mission: [████████] 12% to 24% Bone Mass Lost (Dangerous)
30-Month Mission: [████████████████████] 30% to 60% Bone Mass Lost (Catastrophic)The Post-Flight Recovery Deficit
For years, a common misconception persisted that once an astronaut returned to Earth's $1g$ environment, their bones would naturally and fully rebuild themselves back to baseline levels. However, recent highly precise, data-driven studies have thoroughly debunked this assumption.
A landmark study published in Scientific Reports tracked 17 astronauts for a full 12 months after their return from long-duration missions (ranging from 4 to 7 months) aboard the International Space Station (ISS). Using high-resolution peripheral quantitative computed tomography (HR-pQCT) to scan the distal tibia at a microscopic resolution of 61 micrometers, researchers measured the structural changes in three dimensions.
Distal Tibia Scanning Metrics (HR-pQCT):
- Resolution: 61 Micrometers
- Primary Objective: Measure Trabecular Bone Microarchitecture
- Post-Flight Monitoring Period: 12 to 48 MonthsThe study's findings were sobering:
- Incomplete Recovery: Twelve months after returning to Earth, the astronauts' total bone mineral density, cortical bone density, and trabecular bone volume fraction at the distal tibia remained 0.9% to 2.1% below pre-flight values.
- Persistent Deficits: In 9 out of the 17 astronauts scanned, the shinbone density had not recovered at all after a year on Earth. These individuals were left with a permanent deficit equivalent to approximately a decade’s worth of natural age-related bone loss on Earth.
- Irreversible Structural Damage: To explain the nature of this loss, the study's co-author, Dr. Steven Boyd, director of the McCaig Institute for Bone and Joint Health at the University of Calgary, compared the internal structure of bone to the Eiffel Tower:
> "It is as if some of the connecting metal rods that hold the structure up were lost. And when we return to Earth, we thicken up what's remaining, but we don't actually create new rods."
When the microgravity environment causes the body to resorb trabecular bone, the tiny, microscopic cross-braces (trabeculae) that provide structural strength are completely dissolved. Once these structural "rods" are gone, they cannot be rebuilt. The body can only deposit new bone on top of the remaining structures, thickening the remaining walls (cortical bone) while leaving the internal network permanently compromised.
A separate, long-term case study published in July 2025 followed astronauts up to 48 months (4 years) post-flight. It confirmed that while one of the subjects achieved full recovery, the second subject exhibited persistent, long-term trabecular deficits that were only partially offset by cortical thickening.
The mechanical weakening of the bone actually exceeded the loss of its density. Micro-finite element simulations of the scans revealed that failure loads (the point at which the bone fractures under stress) decreased by 7.45% to 7.49%, even when total density losses appeared far less severe.
The Microscopic Battlefield: Cellular Remodeling and IL-6 Signaling
To understand why the human body destroys its own structural framework in space, scientists must look closely at the cellular mechanics of bone remodeling.
The skeleton is a highly dynamic, living organ. Throughout a person's life, bone tissue is continuously being broken down and rebuilt in a highly coordinated, two-step process called bone turnover. This process is governed by two primary cell types:
- Osteoclasts: Specialized, multinucleated cells derived from hematopoietic stem cells that secrete acid and enzymes to dissolve old or damaged bone tissue (bone resorption).
- Osteoblasts: Mononucleated cells derived from mesenchymal stem cells that synthesize and deposit a collagen-rich osteoid matrix, which subsequently mineralizes with calcium and phosphate to form new bone (bone formation).
On Earth, in a healthy adult under $1g$, the activities of osteoclasts and osteoblasts are tightly coupled and balanced. The rate of bone resorption is perfectly matched by the rate of bone formation, resulting in a stable skeletal mass.
Earth (1g Balance):
[Osteoclast Resorption Rate] == equals == [Osteoblast Formation Rate]
Skeletal Mass = 100% (Stable)
Orbit (0g Imbalance):
[Osteoclast Resorption Rate] >>>> exceeds >>>> [Osteoblast Formation Rate]
Skeletal Mass = Rapidly Decreasing (~1.5% Loss per Month)In microgravity, this homeostatic balance is completely upended. The mechanical unloading of the skeleton causes a severe, immediate down-regulation of osteoblast activity, while osteoclasts continue to break down bone tissue at their normal, terrestrial pace.
According to high-resolution time-lapsed bone scans of astronauts, the rate of bone resorption in microgravity is, on average, three times higher than the rate of bone formation (with bone resorption fractions reaching $2.5\% \pm 2.2\%$ of total bone volume, while formation fractions lag far behind).
Mesenchymal Stem Cell Diversion
At the heart of this osteoblast failure lies a cellular identity crisis occurring deep within the bone marrow. Bone marrow contains a population of multipotent cells known as Bone Marrow Mesenchymal Stem Cells (BMSCs). These stem cells have the potential to differentiate into several distinct lineages, including bone-forming osteoblasts and fat-producing adipocytes (fat cells).
Under normal $1g$ conditions, mechanical strain on the skeleton upregulates a critical transcription factor known as Runx2 (runt-related transcription factor 2, also known as Cbfa1). The activation of Runx2 commits the mesenchymal stem cells to differentiate into osteoblasts, ensuring a steady supply of bone-forming cells to maintain skeletal strength.
In microgravity, the complete lack of mechanical loading suppresses Runx2 and its downstream mitogen-activated protein kinase (MAPK) signaling pathways. Instead, the mechanical unloading upregulates a competing transcription factor called PPARγ2 (peroxisome proliferator-activated receptor gamma 2).
PPARγ2 is the master regulator of fat cell development. As a result, the stem cells that would normally become bone-building osteoblasts are diverted into becoming fat cells.
This shift causes a dual blow to the skeletal system:
- Osteoblast Starvation: The pool of active osteoblasts drops, halting the body's ability to deposit new bone matrix.
- Fat Accumulation: The bone marrow cavity begins to fill with fat tissue, a phenomenon known as marrow adipose tissue expansion.
This cellular shift mimics the natural effects of severe aging and osteoporosis on Earth.
BMSC Differentiation Pathways:
┌───> [Runx2/Cbfa1 Upregulated] ───> Osteoblasts (Bone Tissue)
│ (Activated by 1g Mechanical Load)
Mesenchymal ─────┤
Stem Cells (BMSC)│
└───> [PPARγ2 Upregulated] ────────> Adipocytes (Marrow Fat)
(Activated by 0g Unloading)The IL-6 Signaling Pathway
To make matters worse, microgravity also triggers an inflammatory environment that actively accelerates bone destruction. Research from NASA's Microgravity Associated Bone Loss-B (MABL-B) investigation, which launched to the ISS in April 2026, focuses on a specific protein called Interleukin-6 (IL-6).
IL-6 is a pleiotropic cytokine that plays a major role in systemic inflammation and bone remodeling. Data collected from previous orbital cell-culture experiments suggest that microgravity promotes a specific type of IL-6 signaling that acts as a powerful stimulant for osteoclast cells.
When IL-6 binds to its receptors on surrounding bone cells, it triggers a signaling cascade that upregulates the expression of RANKL (Receptor Activator of Nuclear Factor $\kappa B$ Ligand). RANKL is the primary biochemical signal that instructs precursor cells to mature into active, bone-devouring osteoclasts.
The MABL-B experiment cultured human mesenchymal stem cells alongside osteoclasts for 19 days aboard the ISS to test targeted pharmacological compounds designed to block this IL-6 pathway. By finding a way to interrupt this cellular signal, scientists hope to slow down the rate of bone resorption, providing a key tool to protect astronauts from bone loss during long missions.
The Deep-Space Projections: Mars and the 30-Month Skeletal Crisis
Why are space agencies like the CMSA and NASA suddenly so focused on testing the absolute limits of human physiology with one-year orbital stays? The answer lies in the harsh mathematical realities of deep-space exploration—specifically, a crewed mission to Mars.
Under current chemical propulsion capabilities, a round-trip mission to Mars is constrained by orbital mechanics to a launch window that opens roughly once every 26 months. A typical mission profile requires:
- Outbound Transit: Approximately 9 months (270 days) of deep-space microgravity exposure.
- Surface Stay: Approximately 12 months (365 days) on the Martian surface under a partial gravity of $0.38g$.
- Inbound Transit: Another 9 months (270 days) of microgravity exposure returning to Earth.
This represents a cumulative mission duration of roughly 30 months (900 days), with at least 18 months spent in complete weightlessness and 12 months spent in a severely reduced gravity environment.
Typical Mars Mission Timeline (30 Months Total):
[Outbound Transit: 9 Months 0g] ──> [Surface Stay: 12 Months 0.38g] ──> [Inbound Transit: 9 Months 0g]The Bone Loss Projection
If an astronaut has an average monthly bone loss of 1.5% in their hip and vertebrae, and does not have access to effective countermeasures, the cumulative effect over a 30-month Mars mission is catastrophic:
$$\text{Projected Bone Loss} = 1.5\% \text{ loss/month} \times 18 \text{ months (weightless)} = 27\% \text{ total skeletal decay}$$
This calculation assumes a linear rate of loss, but even with a conservative estimate, an astronaut would lose 30% to 60% of their original bone mineral density in weight-bearing areas.
A 30% reduction in skeletal mass is a critical threshold. On Earth, a loss of this scale would cause severe osteoporosis, leaving the skeleton highly fragile and prone to fractures under minimal stress.
An astronaut returning to Earth or landing on Mars with a skeleton degraded by 30% to 60% would face a major risk of spontaneous spinal or hip fractures from the mechanical loads of normal walking and movement. The bones would simply lack the structural integrity to support the body, rendering the crew physically unable to carry out their mission.
Percentage of Original Bone Mineral Density (BMD) Remaining:
Pre-Flight: [████████████████████] 100% (Healthy)
6-Month ISS: [██████████████████] 90% (Manageable)
One-Year Stay: [████████████████] 80% (High-Risk Threshold)
Mars No Defence: [██████████] 50% (Catastrophic Structural Failure)The Radiation Multiplier
Compounding this skeletal risk is the severe radiation environment of deep space. Unlike astronauts on the ISS or Tiangong, who are partially shielded by Earth's magnetosphere, deep-space travelers are exposed to continuous cosmic rays and solar particle events.
A round-trip Mars mission is calculated to deliver an estimated cumulative radiation dose of 0.66 Sieverts (660 mSv). For comparison, the career limit for most astronauts is around 1.0 Sievert.
This ionizing radiation is not just a cancer risk. High-energy cosmic rays actively damage the highly sensitive bone marrow environment, which is home to the hematopoietic stem cells that produce the body's blood cells, osteoclasts, and osteoblasts.
Exposure to space radiation has been shown to:
- Accelerate Osteoclastogenesis: Ionizing radiation triggers oxidative stress in bone tissues, releasing reactive oxygen species (ROS) that stimulate osteoclasts, leading to accelerated bone resorption.
- Suppress Osteoblast Precursors: Radiation damages the DNA of bone marrow stem cells, triggering cell death and halting their ability to divide into new osteoblasts.
The combination of zero gravity and deep-space radiation creates a destructive cycle. The lack of gravity suppresses bone formation, while cosmic radiation accelerates bone resorption, making deep-space bone loss a major hurdle for Mars exploration.
The Shield: Biomechanical Machines and Pharmaceutical Defenses
To counter these severe physiological changes, space agencies have developed an array of physical and chemical countermeasures. These interventions have successfully reduced bone loss to manageable levels on six-month missions, but a one-year stay will test their effectiveness to the limit.
The Biomechanical Shield: Heavy-Load Resistance
On Earth, human bones are subjected to large mechanical forces from gravity and physical activity. To simulate these loads in space, astronauts must engage in a grueling, mandatory daily exercise program.
Aboard the ISS, the primary tool for this is the Advanced Resistive Exercise Device (ARED). ARED uses a pair of adjustable vacuum cylinders that can generate up to 600 pounds (2,600 Newtons) of constant, load-bearing resistance on the body.
ARED Performance Specifications:
- Resistance Mechanism: Dual Flywheels and Vacuum Cylinders
- Maximum Load Capacity: 600 lbs (2,600 Newtons)
- Mandatory Daily Usage: 2.0 to 2.5 HoursThis device allows astronauts to perform heavy compound exercises, such as:
- Squats
- Deadlifts
- Heel raises
- Overhead presses
By loading the spine and hip joints with forces that mimic Earth's gravity, ARED helps signal the body to maintain its bone density.
The 2022 Scientific Reports study highlighted the importance of these exercises. It found that heavy resistive training, specifically deadlifting, was significantly more effective at preserving bone mass and maintaining the density of the tibia than cardiovascular exercises like running on the T2 Treadmill or riding the Cycle Ergometer.
Even with 2.5 hours of daily training, however, exercise alone cannot completely prevent bone loss, particularly in the internal, spongy trabecular bone compartments.
Average Mechanical Force Generated on Joints:
- Running in Space (T2 Treadmill): ~1.0 to 1.5 times Body Weight
- Heavy Deadlifting (ARED): ~2.5 to 3.5 times Body Weight (Superior Osteogenic Stimulus)The Pharmaceutical Shield: Bisphosphonates
To address the limitations of exercise alone, space agencies have turned to bone-preserving medications. The primary drugs of choice are bisphosphonates, a class of medications widely used on Earth to prevent and treat osteoporosis in postmenopausal women and elderly patients.
Bisphosphonates, such as alendronate (commonly sold under the brand name Fosamax) and zoledronic acid, work by targeting the cells that break down bone. These drugs bind directly to the mineral surface of the bone tissue.
When osteoclast cells begin to resorb and dissolve the bone, they internalize the bisphosphonate molecules. Once inside the cell, the drug disrupts key metabolic pathways, halting the cell's ability to resorb bone and ultimately triggering its self-destruction (apoptosis).
Bisphosphonate Action Mechanism:
[Drug Ingested] ──> [Binds to Bone Mineral Surface] ──> [Osteoclast Resorbs Bone]
──> [Osteoclast Internalizes Drug] ──> [Metabolic Disruption] ──> [Osteoclast Apoptosis (Death)]A major, multi-year joint study conducted by NASA and the Japan Aerospace Exploration Agency (JAXA) evaluated the combined effects of drug therapy and exercise. The study followed a cohort of ISS astronauts who took a weekly oral dose of 70 mg of alendronate, starting three weeks before launch and continuing throughout their six-month missions, while maintaining their standard ARED exercise program.
The results of this dual approach were highly successful:
- Prevention of Bone Loss: The combination of alendronate and ARED exercise prevented declines in bone mineral density in nearly all measured regions of the hip, spine, and pelvis.
- Protection of Internal Structure: Quantitative computed tomography (QCT) scans showed that the drug-and-exercise regimen successfully protected the inner, spongy trabecular bone compartment, which exercise alone had failed to preserve.
- Suppression of Bone Decay Markers: Urinalysis and blood tests of the treated astronauts showed a significant reduction in biochemical markers of bone resorption, indicating that the drug had successfully slowed the hyperactive osteoclast activity in space.
Skeletal Outcome Metrics (Exercise alone vs. Combined Therapy):
ARED Exercise Alone:
- Lumbar Spine BMD: Slighly Attenuated (partial loss)
- Hip Trabecular BMD: Persistent Decline (-4% to -8%)
- Bone Resorption Markers: Elevated (high decay)
ARED + Bisphosphonates (Alendronate):
- Lumbar Spine BMD: Fully Preserved (or slight gain)
- Hip Trabecular BMD: Preserved (near-zero loss)
- Bone Resorption Markers: Suppressed to normal Earth levelsHowever, bisphosphonates are not a perfect solution. They are resorption inhibitors; they work by stopping the breakdown of bone, but they do not actively stimulate the formation of new, healthy bone tissue.
Additionally, long-term use of bisphosphonates carries risks. Over years of continuous use, these drugs can over-suppress the body's natural bone remodeling process, leading to micro-cracks in the skeleton that cannot heal, increasing the risk of atypical fractures.
The Next Generation: NELL-1 and Stem Cell Therapies
To overcome these limitations, researchers are developing next-generation drugs designed to actively promote bone growth in weightless environments.
One of the most promising candidates is a modified protein compound known as BP-NELL-PEG. Engineered by a research team at the Forsyth Institute and tested on mice aboard the ISS, this compound combines the bone-building protein NELL-1 with a PEGylated bisphosphonate.
Unlike traditional bisphosphonates, which only stop bone resorption, BP-NELL-PEG is designed to target the bone surface and actively stimulate osteoblast cells to build new bone tissue, even in the absence of gravitational loads.
The animal trials on the ISS showed promising results, demonstrating a significant increase in bone formation with no observable side effects. This and similar therapies are now being evaluated for future human missions.
The Geopolitical and Technological Race to the Lunar Surface
The launch of the Shenzhou-23 mission and its planned one-year orbital stay occurs against the backdrop of an accelerating, high-stakes space race between the world’s major space powers.
The United States, through its Artemis program, is working to establish a sustainable human presence on the Moon. NASA’s Artemis II mission, which sent a crew of four on a flight path around the Moon, marked the first crewed lunar flight in over half a century.
Meanwhile, China’s space program is advancing rapidly, aiming for its first crewed lunar landing before 2030.
Geopolitical Race to the Moon:
United States (Artemis Program):
- Goal: Establish sustainable lunar orbital and surface presence.
- Current Milestones: Artemis II crewed flyby completed.
- Next Steps: Artemis III crewed landing.
China (Manned Lunar Program):
- Goal: Crewed lunar landing before 2030.
- Current Milestones: Shenzhou-23 rapid docking and 1-year physiological stress test.
- Next Steps: Mengzhou spacecraft orbital flight tests in 2026.To achieve its 2030 goal, China is currently developing and testing entirely new classes of hardware and launch infrastructure:
- Long March 10: A heavy-lift rocket designed to launch crewed spacecraft and landers to the Moon.
- Mengzhou Spacecraft: China's next-generation crewed capsule, designed to replace the aging Shenzhou line, with its first orbital flight test scheduled for 2026.
- Lanyue Lunar Lander: The spacecraft designed to carry two astronauts from lunar orbit down to the surface of the Moon.
But building powerful rockets and spacecraft is only half of the challenge. A successful moon landing hinges on the survival and performance of the crew.
Astronauts traveling to the Moon will face a transition from the relative safety of low-Earth orbit to a much more demanding, partial-gravity environment. Unlike the ISS or Tiangong, which are located just hours away from emergency medical evacuation to Earth, a crew on the Moon will be days away from medical help. A crew on Mars will have no evacuation option at all.
Emergency Evacuation Times to Earth:
- Low Earth Orbit (ISS/Tiangong): ~3 to 6 Hours
- Lunar Surface (Artemis/ILRS): ~3 to 5 Days
- Martian Surface: No Evacuation Option (30-Month Commitment)If an astronaut arrives at the Moon or Mars with their skeleton severely weakened by microgravity, they could suffer a debilitating fracture during a routine surface walk. This risk makes understanding and preventing bone loss a primary operational requirement for deep-space exploration.
The one-year mission on the Shenzhou-23 flight will provide Chinese scientists with crucial, long-term physiological data. By studying how a Chinese astronaut adapts to a full year in microgravity, the CMSA can validate its own exercise machines, medical systems, and drug therapies.
This data will allow mission planners to customize physical training and medical regimens for individual astronauts, helping to ensure that when they finally step onto the lunar surface, their skeletons will be strong enough to handle the mission.
Looking Ahead: The Frontiers of Space Medicine
As the Shenzhou-23 crew begins their long stay aboard the Tiangong space station, scientists and mission planners around the world will be watching their progress closely.
Over the next 12 months, the astronaut selected for the extended stay will undergo regular, detailed health monitoring. This will include periodic bone densitometry scans, blood and urine tests, cardiovascular checks, and cognitive assessments.
These tests will track the exact, month-by-month changes in their body, providing a detailed record of how the human skeleton adapts to a year in weightlessness.
Shenzhou-23 One-Year Flight Path:
- Launch & Docking: May 24, 2026 (Completed)
- Physiological Testing: Every 30 Days (BMD, Biometrics)
- Mission Handover: Late 2026 (Shenzhou-24/25 Rotations)
- Scheduled Landing: May 2027While these studies are designed to support deep-space exploration, the findings will also have major benefits for healthcare on Earth.
The cellular and chemical pathways that drive bone loss in space are the same ones that cause osteoporosis in millions of aging people on Earth. By studying how to block these pathways in the extreme environment of microgravity, scientists can develop more effective drugs and treatments to fight bone diseases on Earth.
For the crew of Shenzhou-23, the next 365 days will be a demanding test of physical and mental endurance. Their mission represents a crucial step forward for human spaceflight, helping to build the physiological foundation that will allow future travelers to leave Earth's orbit and explore the solar system.
Reference:
- https://www.khaosodenglish.com/news/international/2026/05/25/china-launches-shenzhou-23-mission-sending-one-astronaut-for-year-long-stay/
- https://www.japantimes.co.jp/news/2026/05/25/asia-pacific/china-space-flight-moon/
- https://www.channelnewsasia.com/east-asia/china-astronaut-year-long-space-mission-2030-moon-landing-6138496
- https://www.theguardian.com/world/2026/may/24/china-launches-three-crew-space-flight-moon-shenzhou-23-mission
- https://www.cbsnews.com/news/china-launches-shenzhou-spacecraft-astronauts/
- https://www.thestandard.com.hk/china/article/332816/China-to-send-astronaut-on-year-long-space-mission-as-it-eyes-2030-moon-landing
- https://www.nasa.gov/reference/risk-of-spaceflight-induced-bone-changes/
- https://english.news.cn/20260523/84a32f8316c74773b88ee3eb1176c533/c.html
- https://supercarblondie.com/how-nasa-astronaut-frank-rubios-body-changed-after-more-than-a-year-in-space/
- https://primeview.co/the-impact-of-long-term-space-travel-on-the-human-body-insights-from-frank-rubios-371-day-mission/
- https://pubmed.ncbi.nlm.nih.gov/31400472/
- https://medicine.iu.edu/blogs/spirit-of-medicine/record-space-flight-inspires-bone-research-at-iu-school-of-medicine
- https://spacedaily.com/d-astronauts-on-the-iss-lose-about-1-2-of-their-bone-density-per-month-in-microgravity-meaning-a-six-month-mission-costs-them-as-much-bone-mass-as-a-postmenopausal-woman-loses-in-a-year/
- https://spacedaily.com/d-astronauts-on-the-iss-lose-about-1-2-of-their-bone-density-per-month-in-microgravity-meaning-a-six-month-mission-costs-them-as-much-bone-mass-as-a-postmenopausal-woman-loses-in-a-year/
- https://learningenglish.voanews.com/a/study-drug-could-block-bone-loss-in-astronauts-in-space/7278803.html
- https://www.sciencealert.com/new-study-reveals-devastating-effect-on-astronaut-bones-from-being-in-space
- https://pmc.ncbi.nlm.nih.gov/articles/PMC11661419/
- https://digitalcommons.library.tmc.edu/cgi/viewcontent.cgi?params=/context/baylor_docs/article/4721/&path_info=cells_13_01337.pdf
- https://pmc.ncbi.nlm.nih.gov/articles/PMC12304210/
- https://www.researchgate.net/publication/261256987_Physiological_Effects_of_Microgravity_on_Bone_Cells
- https://pmc.ncbi.nlm.nih.gov/articles/PMC6496371/
- https://www.nasa.gov/missions/station/iss-research/counteracting-bone-and-muscle-loss-in-microgravity/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC2971652/
- https://academic.oup.com/endo/article/145/5/2421/2878328
- https://en.wikipedia.org/wiki/Human_mission_to_Mars
- https://pmc.ncbi.nlm.nih.gov/articles/PMC10178040/
- https://pubmed.ncbi.nlm.nih.gov/23334732/
- https://www.thehindu.com/news/international/china-to-send-astronaut-on-year-long-space-mission-as-it-eyes-2030-moon-landing/article71015852.ece